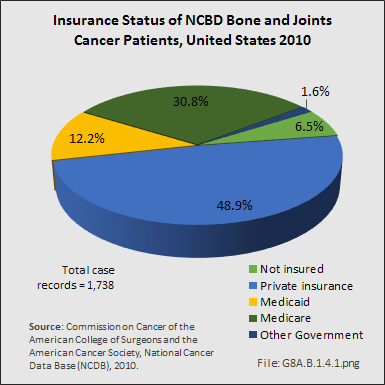
From 1998–2010, information on insurance coverage was available for roughly 96% of patients treated with soft tissue sarcomas. The largest insurance payer was managed care (33%), followed by Medicare with supplement (25%). Private insurance accounted for 14%, while Medicare (11%) accounted for a larger percentile than Medicaid (5%). Detailed NCDB insurance data for 7,684 of 7,878 cases of soft tissue sarcoma reported from the year 2010 showed private insurance paying just over 46%, while Medicare/Medicaid paid a slightly larger share of 47%.1

The total economic costs of malignant soft tissue sarcoma are unknown. Surgery is often the first line of treatment for soft tissue sarcoma. Multiple therapies may be needed later in the course of the patient’s disease, especially in the more advanced cases. In the later stages of the disease in those not cured with surgery alone, significant costs will accumulate as the patients develop pulmonary disease and ultimately die. Hormone therapy, immunotherapy, and bone marrow transplant/endocrine treatments are undertaken in a small number of cases that fail standard treatments. Overall, costs will vary with treatments utilized, number and intensity of treatments, and can easily top $100,000 for a single patient that receives surgery, chemotherapy, and radiation therapy.
Throughout the years 2005–2008, one study reported that the average professional charge for a primary excision was $9,700 and $12, 900 for re-excision. Although every 1-cm increase in size of the tumor results in an increase of $148 for a primary excision, size was not an independent factor affecting re-excision rates. The grade of the tumor was positively associated with professional charge, such that higher-grade tumors resulted in higher charges compared to lower-grade tumors. Analysis including professional technical and indirect charges revealed that, on average, patients undergoing definitive primary excision at their cancer treatment center were charged $40,230. This was compared to $44,770 for to patients receiving definitive re-excision of unsuccessful or incomplete previous resections at the same cancer treatment center. This higher cost did not include the charges and costs generated by their previous unsuccessful or incomplete previous attempt at resection.2
This analysis confirms that proper work-up, evaluation, and treatment are key to maintain costs, as well as, hopefully, improving the outcome for these patients. This cost analysis did not include the costs associated with chemotherapy or radiation therapy, or the costs of diagnostic and follow-up laboratory and radiographic studies, nor the actual costs of care.
- 1. Commission on Cancer of the American College of Surgeons and the American Cancer Society, National Cancer Data Base (NCDB), 2010.
- 2. Alamanda VK, Delisca GO, Mathis SL, et al: The financial burden of re-excising incompletely excised soft tissue sarcomas: A cost analysis. Ann Surg Oncol 2013:(9):2808-2814.
Edition:
- 2014
 Download as CSV
Download as CSV